
Design thinking in healthcare isn’t a workshop exercise. It’s the difference between building technology patients actually use and building technology that collects dust. When Children’s Hospital Los Angeles needed to solve NICU discharge, where overwhelmed parents forget 40-80% of clinical instructions within a week, they didn’t start with a requirements document. They started by sitting with families and watching what happened when a nurse handed over a stack of paperwork to a mother who hadn’t slept in three days.
Healthcare Implementations
(14 Years)
Clutch Rating
(48+ Reviews)
Inc 5000 + Design
Award Winners
Last updated: May 2026
By: Kevin Yamazaki, Partner, CEO at Sidebench
In this article:
- What is design thinking in healthcare?
- Why does healthcare need a different design approach?
- What are the five phases of healthcare design thinking?
- How did CHLA use design thinking for NICU families?
- How did UCSF map the patient journey for stroke care?
- How did Peer Health Exchange design selfsea for adolescents?
- How did IEHP scale from 1,000 to 90,000 users?
- Where did Sidebench’s design thinking practice come from?
- What mistakes do healthcare organizations make with design thinking?
- How do you start a design thinking project in healthcare?
- Key takeaways
- FAQ
What is design thinking in healthcare?
Design thinking is a problem-solving methodology that starts with the people who’ll actually use what you build, patients, clinicians, administrators, before writing a single line of code. In healthcare, this means observing real clinical workflows, mapping patient journeys across fragmented systems, and prototyping solutions that survive contact with the realities of shift changes, HIPAA constraints, and insurance authorization workflows.
Tim Brown, CEO of IDEO, describes it as bringing together “what is desirable from a human point of view with what is technologically feasible and economically viable.” That’s a clean definition. But in healthcare, there’s a fourth dimension most industries don’t face: regulatory compliance. Every design decision has to hold up against HIPAA, FDA, CMS, and state-level requirements simultaneously.
The payoff is real. The Design Management Institute tracked design-led companies over ten years and found they outperformed the S&P 500 by 219% (DMI Design Value Index, 2015). In healthcare specifically, a 2019 study in the Journal of Medical Internet Research found that human-centered design approaches increased patient engagement with digital health tools by 60% compared to technology-first approaches.
Why does healthcare need a different design approach?
Healthcare has constraints that consumer tech doesn’t: clinical workflows can’t be disrupted mid-procedure, data handling is legally regulated, and the end user is often someone in pain, scared, or cognitively overloaded. A design thinking process built for a fintech app won’t survive its first day in an emergency department.
Here’s what makes healthcare different from every other industry:
| Factor | Consumer Tech | Healthcare Tech |
|---|---|---|
| User state | Relaxed, browsing | Stressed, time-constrained, possibly in pain |
| Stakeholders | User + buyer (often same person) | Patient + clinician + admin + payer + regulator |
| Data handling | GDPR/CCPA | HIPAA + state laws + CMS + FDA (if SaMD) |
| Failure cost | Lost revenue, churn | Patient harm, regulatory fines, malpractice exposure |
| Integration | APIs, third-party services | EHR systems (Epic, Cerner), HL7/FHIR, legacy infrastructure |
| Testing | A/B test in production | Sandbox environments, IRB approval for clinical testing |
The multi-stakeholder problem is the one that kills most healthcare technology projects. You’re not designing for one user. You’re designing for a nurse who has 12 seconds between patients, a parent who can’t remember what the doctor said, an administrator who needs compliance documentation, and an insurance company that needs specific billing codes. Get any one of those wrong and adoption collapses.
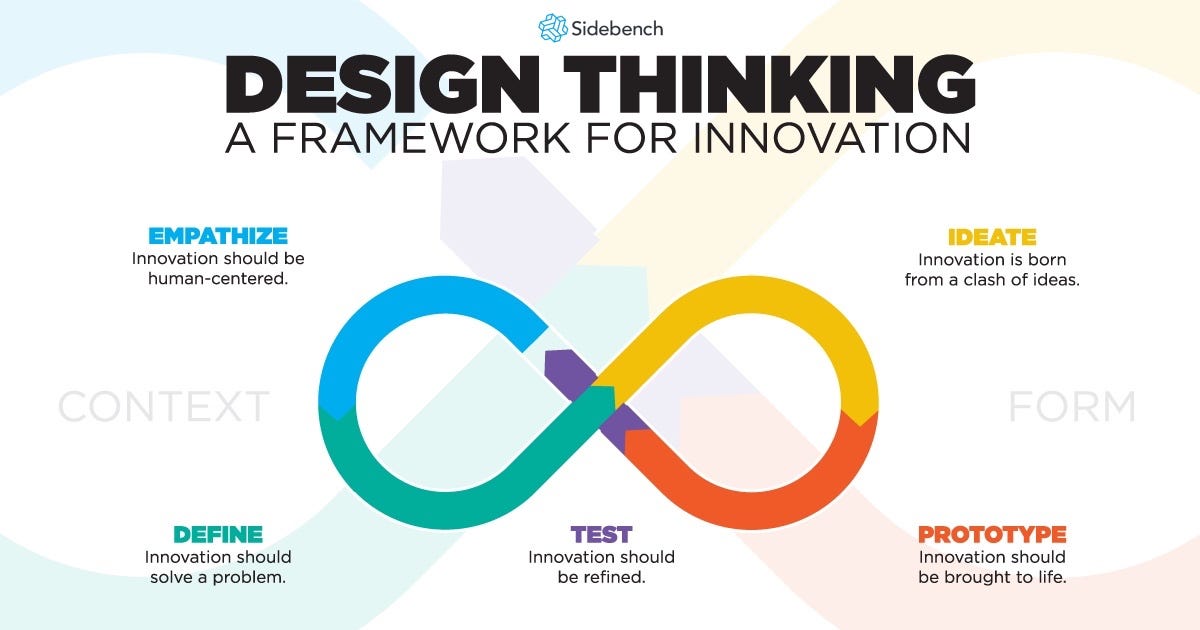
What are the five phases of healthcare design thinking?
The five phases, empathize, define, ideate, prototype, test, stay the same as general design thinking. But in healthcare, each phase has specific methods and constraints that change how the work actually gets done.
1. Empathize: clinical observation, not just user interviews
In consumer tech, you can run a survey. In healthcare, you need to stand in the room. We call this “clinical shadowing”, spending time in the actual environment where your technology will live. You watch the workarounds. The sticky notes on monitors. The whiteboard that’s actually running the unit’s scheduling because the EHR can’t handle it.
At CHLA, our team observed NICU discharge meetings, WIC program interactions, and Social Security Administration visits. We ran focus groups with parents and caregivers, generating roughly 200 data points that we organized through affinity diagramming. None of this shows up in a requirements document sent over email.
2. Define: map the journey across systems, not screens
Healthcare journeys don’t live inside one application. A behavioral health patient might interact with an intake system, a scheduling platform, a telehealth tool, an EHR, and a billing system in a single episode of care. The design thinking “define” phase needs to map this entire journey, including the gaps between systems where patients and data get lost.
3. Ideate: within constraints, not despite them
Here’s where healthcare design thinking separates from the generic version. You can’t ideate solutions that violate HIPAA. You can’t prototype features that require access to PHI without proper authorization workflows. The constraints aren’t limitations, they’re design parameters. The best healthcare solutions are the ones that make compliance invisible to the user.
4. Prototype: paper first, code last
We’ve seen organizations jump straight to building a working application. That’s a $200K mistake when you discover the clinical workflow doesn’t match your assumptions. Paper prototypes, clickable mockups, and simulated workflows cost almost nothing to test and iterate. Save the engineering budget for when you know what you’re building.
5. Test: with real users in real clinical settings
Testing a healthcare application with internal QA isn’t testing. Real testing means putting a prototype in front of a nurse during a shift, a patient in a waiting room, an administrator processing authorizations. The feedback you get in these contexts is fundamentally different from what you get in a conference room demo.
How did CHLA use design thinking for NICU families?
Children’s Hospital Los Angeles partnered with Sidebench to build Baby Steps LA, an app that supports NICU families through discharge and post-discharge care. The project started with clinical observation, not a product spec, and has since supported over 17,000 families with a 4.7-star satisfaction rating.
The core insight came from observation, not assumptions. Parents in NICU discharge meetings were receiving complex medication schedules, specialist referrals, and warning signs to watch for, all while emotionally overwhelmed. Research shows patients forget 40-80% of medical information immediately, and nearly half of what they do remember is incorrect (Kessels, 2003).
The design thinking solution wasn’t to digitize the discharge paperwork. It was to rethink the entire information delivery model:
- Curated content library, CHLA-approved resources that nurses help families select during discharge, specific to their baby’s diagnosis
- Baby profile, stores diagnosis, physicians, and medications so parents can reference details when talking to multiple care teams
- Interactive checklists, post-discharge action items organized as to-do lists, replacing the overwhelming paper handouts
30,000+ downloads. 17,000+ families supported. That’s what design thinking looks like when it’s done right in healthcare.
How did UCSF map the patient journey for stroke care?
The UCSF Clinical Innovation Center partnered with Sidebench on a stroke patient journey mapping engagement that surfaced where the clinical system was actually losing time, and patient outcomes, between symptom onset and treatment.
Stroke care is a discipline where minutes matter and the operational chain is long: 911 call, EMS triage, emergency department arrival, imaging, neurology consult, treatment decision, transfer if needed. Each handoff introduces friction. Mapping the journey end-to-end, from the patient’s perspective and from each clinician’s perspective, exposes the bottlenecks that no individual care team can see from inside their part of the workflow.
The pattern from this kind of work: when you map the actual journey rather than the assumed one, you find the leverage points where small workflow or technology changes can move outcomes that no amount of additional clinical effort would shift on its own.
How did Peer Health Exchange design selfsea for adolescents?
Peer Health Exchange (PHE) and Sidebench co-designed selfsea, a digital mental-health platform for adolescents, that earned a Fast Company Innovation by Design honor, a w3 Award, and Common Sense Media’s 4-star rating. The platform has reached over 700,000 young people, with more than 1 million minutes of mindfulness delivered through a Headspace integration.
Designing for adolescents is its own discipline. Stigma, trust, language, identity, and privacy all behave differently in this population than in adult clinical contexts. selfsea’s design process leaned into participatory design with young people, not for them. Teen advisors shaped the content categories, the tone, and the way the app handled identity and disclosure. The result is a product young users actually open without being told to.
What design thinking added: a process that treated the target users as collaborators in the build, not subjects of it. That’s the difference between a digital health product that wins awards and one that wins usage.
How did IEHP scale from 1,000 to 90,000 users?
Inland Empire Health Plan (IEHP) partnered with Sidebench to build a member engagement platform that grew from 1,000 to 90,000 active users, processing 2 million transactions annually, serving a predominantly Medicare-Medicaid population in Southern California.
The design challenge was specific: IEHP’s member population includes significant non-English-speaking communities, varying levels of digital literacy, and members who often navigate complex benefits across both Medicare and Medicaid simultaneously. A generic patient portal wasn’t going to work.
Design thinking uncovered that members weren’t struggling with the technology itself. They were struggling with understanding their benefits. The solution focused on personalized benefits navigation, showing each member exactly what they’re eligible for, in their language, with clear next steps. Not a feature list. A human-centered information architecture.
| Project | Design Insight | Outcome |
|---|---|---|
| CHLA Baby Steps | Parents can’t absorb info during NICU discharge | 17,000+ families supported; 4.7-star rating; American Hospital Association Innovation Challenge 2019; Fast Company Best Mobile Apps |
| UCSF Clinical Innovation Center | Stroke care loses time and outcomes between symptom and treatment | Patient journey mapping that drove operational redesign, not just product redesign |
| Peer Health Exchange / selfsea | Adolescents won’t open generic mental health apps | 700K+ young people reached; 1M+ minutes of mindfulness via Headspace; Fast Company Innovation by Design Honoree; w3 Award; Common Sense Media 4-star |
| IEHP Platform | Members struggle with benefits across Medicare and Medicaid | 1K to 90K users in months without significant marketing spend; 3M digital transactions/year |
Four different organizations. Four different problems. Same approach: start with the people, not the technology.
What mistakes do healthcare organizations make with design thinking?
The biggest mistake is treating design thinking as a one-time workshop instead of an ongoing methodology. We’ve seen organizations run a two-day design sprint, declare victory, and then hand a list of features to engineering with zero user validation. That’s not design thinking. That’s brainstorming with sticky notes.
Other mistakes we see consistently:
- Skipping clinical observation. Interviewing stakeholders in a conference room isn’t the same as watching them work. The workarounds are invisible until you’re in the environment.
- Designing for one user type. A patient portal that works for patients but makes nurses’ jobs harder won’t get adopted. Healthcare technology serves multiple stakeholders simultaneously.
- Ignoring compliance during ideation. “We’ll add HIPAA later” is a statement that costs organizations months of rework. Compliance needs to be a design parameter from day one, not an afterthought.
- Over-prototyping. A clickable mockup should test a hypothesis, not demonstrate engineering capability. If your prototype takes three months to build, you’ve gone too far before validating.
- Not testing with real clinical environments. A demo in a boardroom tells you nothing about whether your solution works during a 7am shift change.
How do you start a design thinking project in healthcare?
Start with a specific problem, not a technology solution. “We need an app” isn’t a design brief. “Our NICU parents forget 80% of discharge instructions within a week” is.
A practical starting point:
- Identify the pain point with the highest cost. Where are patients dropping off? Where are clinicians spending time on workarounds? Where is the organization losing money to inefficiency?
- Get clinical access. You need permission to observe workflows in the actual environment. This requires organizational buy-in, not just IT department approval.
- Assemble a cross-functional team. Clinicians, patients, IT, compliance, and operations should all be represented. Design thinking fails when it’s owned by a single department.
- Set measurable outcomes. “Improve patient experience” is too vague. “Reduce NICU readmission rate by 15% within 6 months” is testable.
- Prototype before you build. Paper mockups, clickable prototypes, simulated workflows. Test your assumptions before committing engineering resources.
Key takeaways
- Healthcare design thinking requires clinical observation, you can’t design for workflows you haven’t witnessed firsthand
- Multi-stakeholder design is non-negotiable, patients, clinicians, administrators, and payers all need to be considered simultaneously
- Compliance is a design parameter, not an afterthought, build HIPAA into the design process from day one
- Start with the problem, not the technology, “our parents forget discharge instructions” beats “we need an app”
- Design-led companies outperform by 219%, the ROI of human-centered design is documented across industries (DMI Design Value Index)
Where did Sidebench’s design thinking practice come from?
Design thinking at Sidebench isn’t a marketing label retrofitted to a build practice. It came from years of teaching, lecturing, and running workshops in healthcare design specifically. Kevin Yamazaki taught a multi-day professional education course on design thinking, guest-lectured on digital health design thinking at the USC graduate program, and co-ran the WITH Foundation accessibility workshops at SXSW. The practice was shaped by working alongside clinicians, patients, and product teams in regulated environments before it was applied to a single Sidebench engagement.
The cross-industry exposure matters. Designing for healthcare benefits from designing for outside-of-healthcare context too: brand partners and consumer products that span Oakley, Red Bull, Sony, NBC Universal, HP, Microsoft, Andreessen Horowitz, and Lightspeed sit alongside the healthcare client roster. Patterns that work in consumer brand and entertainment design transfer into clinical UX in unexpected places, like how stigma-aware adolescent products borrow more from consumer creative than from clinical-IT conventions.
Sidebench perspective
We’ve applied design thinking across 60+ healthcare implementations spanning 14 years, from NICU family support at CHLA to stroke journey mapping at the UCSF Clinical Innovation Center to adolescent mental health on selfsea to member engagement at IEHP. The pattern is consistent: organizations that invest in understanding their users before building technology get better outcomes, faster adoption, and lower long-term costs. The organizations that skip this step and jump straight to development spend more money on rework than they would have spent on research. Design thinking in healthcare is risk mitigation, not luxury.
FAQ
What is design thinking in healthcare?
Design thinking in healthcare is a problem-solving methodology that starts with observing and understanding the people who’ll use a product, patients, clinicians, administrators, before designing or building anything. It follows five phases: empathize, define, ideate, prototype, and test. In healthcare, each phase is adapted for clinical environments, multi-stakeholder needs, and regulatory compliance requirements like HIPAA.
How is design thinking different from traditional healthcare IT project management?
Traditional approaches start with a requirements document and build to spec. Design thinking starts with observation and builds to validated user needs. The practical difference: design thinking projects typically discover 30-40% of requirements during the empathize phase that weren’t in the original brief, reducing rework later in development.
How long does a healthcare design thinking project take?
A discovery and design phase typically takes 4-8 weeks, depending on the complexity of the clinical environment and number of stakeholder groups. This includes clinical observation, user research, journey mapping, ideation, and initial prototyping. The investment in this phase typically reduces overall project timelines by avoiding costly mid-development pivots.
Can you apply design thinking to existing healthcare applications?
Yes. Design thinking is often most valuable when applied to existing applications with poor adoption. Clinical observation and user research can reveal why a platform isn’t being used, often the issue is workflow mismatch rather than missing features. Sidebench has applied this approach to optimize existing platforms at organizations like IEHP, where design-led improvements helped scale from 1,000 to 90,000 active users.
What’s the ROI of design thinking in healthcare?
Design-led companies outperform the S&P 500 by 219% over ten years (DMI Design Value Index). In healthcare specifically, outcomes include reduced readmission rates, improved patient satisfaction scores, higher staff adoption of digital tools, and lower development costs through early validation. CHLA’s Baby Steps achieved a 4.7-star patient satisfaction rating. Cortica’s design-led scheduling platform reduced waitlists from 6 months to under 30 days and now generates $6.7M in annual revenue from AXON.
How does design thinking work with HIPAA compliance?
Compliance becomes a design parameter, not an afterthought. During the ideate and prototype phases, solutions are evaluated against HIPAA Security Rule requirements (45 CFR 164.312) alongside user needs. This means access controls, audit logging, and encryption are designed into the user experience from the start, rather than bolted on after development.
Do you need to hire a design thinking consultant?
Not necessarily for the methodology itself, the five phases are well-documented. But healthcare-specific design thinking requires clinical access, HIPAA expertise, and experience with EHR integrations that most internal teams don’t have. Organizations building patient-facing or clinician-facing technology typically benefit from a partner who’s done this in regulated environments before.
What industries use design thinking besides healthcare?
Design thinking originated in industrial design (IDEO, Stanford d.school) and is now standard practice in financial services, education, government, and consumer technology. Healthcare adopted it later than most industries because of regulatory complexity, but organizations like Mayo Clinic, Kaiser Permanente, and Cincinnati Children’s have built internal design thinking capabilities.
How do you measure the success of a design thinking project?
Define measurable outcomes before you start. In healthcare, common metrics include: patient satisfaction scores, clinical adoption rates, time-to-task completion, readmission rates, patient portal engagement, and operational efficiency gains. Avoid vanity metrics like “number of features shipped”, measure whether people actually use what you build.
What’s the difference between design thinking and UX design?
Design thinking is the problem-solving methodology. UX design is the practice of designing interfaces and interactions. You can do UX design without design thinking (and many organizations do, with predictably poor results). Design thinking without UX execution is just research. The two work together: design thinking tells you what to build, UX design determines how it looks and works.
Can design thinking be applied to behavioral health specifically?
Yes, and it’s particularly valuable because behavioral health workflows are so different from acute care. Session-based scheduling, multi-provider coordination, ongoing insurance authorization, and complex documentation requirements all benefit from a human-centered approach. Sidebench’s work with Cortica and LEARN Behavioral used design thinking to solve scheduling and intake automation challenges specific to behavioral health.
What tools do you use for design thinking in healthcare?
The tools matter less than the process. That said, common tools include: journey mapping software (Miro, FigJam), prototyping tools (Figma, InVision), affinity diagramming (physical sticky notes still work best), and user research platforms for recording and analyzing observation sessions. The critical “tool” is clinical access, the ability to observe real workflows in real environments.
Ready to apply design thinking to your healthcare challenge?
Whether you’re building a new patient-facing application or trying to understand why your current platform has low adoption, the first step is the same: understand the people who’ll use it.
Run a healthcare design-thinking sprint with the team behind Baby Steps and selfsea →
Cited data sources
- Design Management Institute, DMI Design Value Index: design-led companies outperform S&P 500 by 219%
- IDEO / Tim Brown, Design thinking methodology definition
- Kessels, 2003, Patients’ memory for medical information (Journal of the Royal Society of Medicine)
- CHLA Baby Steps LA, Sidebench case study: NICU family support application
- Harvard Business Review, Design Thinking Comes of Age (2015)







