
Communication failures contribute to up to 80% of serious medical errors, according to The Joint Commission. That’s not a soft-skills problem. It’s an architecture problem. When a NICU parent forgets 80% of discharge instructions within a week, the fix isn’t better handwriting on the paperwork. It’s rethinking how information reaches patients in the first place, and that’s where technology enters the picture.
Healthcare Implementations
(14 Years)
Patient Appointments
Annually
Inc 5000 + Design
Award Winners
Last updated: May 2026
By: Kevin Yamazaki, Partner, CEO at Sidebench

In this article:
- Why does patient communication fail in healthcare?
- What does poor patient communication actually cost?
- How is technology changing patient communication?
- What makes a patient communication platform effective?
- How did CHLA solve NICU family communication?
- How does IEHP communicate with 90,000 members across languages?
- What are the biggest patient communication mistakes?
- How do you measure patient communication improvement?
- Key takeaways
- FAQ
Why does patient communication fail in healthcare?
Patient communication fails because healthcare systems were designed around clinical workflows, not patient understanding. Information moves between providers through EHR notes and handoff protocols, but the patient sits at the end of that chain receiving a five-minute verbal summary of complex medical decisions.
The data is striking. CRICO Strategies (Harvard’s risk-management affiliate), in its benchmarking review of malpractice claims, analyzed 23,000 medical malpractice claims and found communication failure was a contributing factor in 30% of cases, accounting for 1,744 patient deaths and $1.7 billion in costs. Of those failures, 53% involved provider-to-patient miscommunication. The other 47% happened between providers themselves.
And patients aren’t retaining what they do hear. Research published in the Journal of the Royal Society of Medicine found patients forget 40-80% of medical information immediately after a clinical encounter. Nearly half of what they remember is incorrect (Kessels, 2003). That’s not a patient problem. It’s a system design problem.
Three factors make healthcare communication uniquely hard:
- Information asymmetry. Clinicians have years of training. Patients are processing unfamiliar terminology while anxious, tired, or in pain.
- Fragmentation. A single episode of care might involve a primary physician, two specialists, a pharmacist, an insurance coordinator, and a scheduler. Each one communicates independently.
- Time pressure. The average primary care visit lasts 18 minutes. That’s not enough to explain a complex diagnosis, review medications, outline next steps, and confirm the patient actually understood.
What does poor patient communication actually cost?
Poor patient communication costs the U.S. healthcare system billions annually through preventable readmissions, malpractice claims, and treatment non-adherence. The Joint Commission’s 2024 data shows sentinel events surged 13% year-over-year, with communication breakdowns cited as a systemic contributing factor.
| Cost Category | Impact | Source |
|---|---|---|
| Malpractice claims | $1.7B from communication failures alone | CRICO Strategies |
| Patient deaths | 1,744 deaths linked to communication errors | CRICO Strategies |
| Sentinel events | 1,575 reported in 2024 (up 13% YoY) | The Joint Commission |
| Data breaches | $9.77M average breach cost | IBM/Ponemon 2024 |
| Documentation failures | 20% of malpractice cases involve documentation errors | CRICO/Candello 2024 |
There’s a less obvious cost, too. When patients don’t understand their care plan, they don’t follow it. They miss medications. They skip follow-up appointments. They show up in the emergency department for something that could have been handled at home. Every readmission within 30 days costs a hospital an average of $15,200 (CMS data), and CMS penalizes hospitals with excessive readmission rates through the Hospital Readmissions Reduction Program.
That penalty creates a direct financial incentive to fix patient communication. But most organizations try to fix it with training programs for clinicians rather than building systems that support better information delivery. Training helps. Systems scale.
How is technology changing patient communication?

Patient communication technology has shifted from simple patient portals to multi-channel platforms that deliver personalized, HIPAA-compliant information through apps, SMS, and telehealth. In 2024, 65% of patients accessed their health records online, up from just 25% a decade ago (ONC/HINTS 2024).
The growth is real but uneven. While 77% of patients were offered online access to their health information in 2024, provider encouragement makes a massive difference: 87% of patients whose provider actively encouraged portal use accessed it, compared to 57% of those whose provider didn’t mention it (ONC/HINTS 2024).
App-based access is growing fastest, from 38% of patients in 2020 to 57% in 2024. That’s a signal. Patients want health information on the device they already carry, not through a browser-based portal they have to remember to check.
But here’s what most patient portal statistics miss. Having a portal and having effective patient communication are two completely different things. A portal that shows lab results without context doesn’t help a patient understand what those results mean. A discharge summary written in clinical terminology doesn’t help a parent manage their child’s medication schedule at home.
Personalization at scale does not require a machine-learning model. For the American Heart Association, we built a behavioral-science personalization engine that segments 1.3 million members into five psychographic groups and maps each to tailored, evidence-based care plans built around the organization’s Life’s Simple 7 framework, all without an ML model. The lesson for patient communication is that disciplined segmentation and behavioral science often outperform algorithmic complexity for engagement.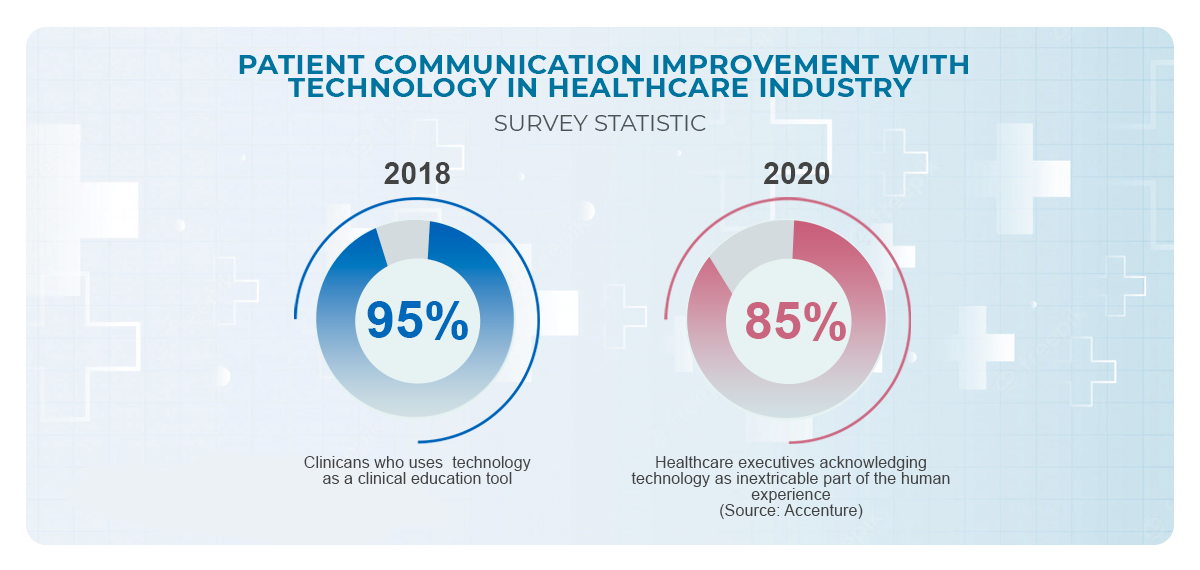
The technology that actually improves patient communication does three things:
- Meets patients where they are. Mobile-first, multilingual, accessible across literacy levels. Not “download our app and create an account” but information delivered through channels patients already use.
- Contextualizes clinical information. Translates medical data into actionable guidance. Not “hemoglobin 10.2 g/dL” but “your iron levels are low, here’s what to eat and when to call us.”
- Closes the loop. Confirms understanding, tracks adherence, and flags when a patient is falling off their care plan before it becomes an emergency department visit.
What makes a patient communication platform effective?

An effective patient communication platform combines HIPAA-compliant messaging, personalized content delivery, multilingual support, and integration with existing EHR systems. The platform has to work inside the clinical workflow, not alongside it, otherwise clinicians won’t use it, and the communication gap stays open.
| Feature | Basic Portal | Purpose-Built Platform |
|---|---|---|
| Content delivery | Static documents, PDFs | Personalized, condition-specific guidance |
| Language support | English-only or basic translation | Native multilingual with cultural context |
| EHR integration | View-only data pull | Bi-directional via HL7/FHIR |
| Engagement model | Patient must log in and check | Push notifications, SMS, in-app reminders |
| Compliance | Portal-level HIPAA | Application-layer HIPAA |
| Outcome tracking | Login counts, page views | Adherence rates, comprehension, engagement scores |
The gap between these two columns is where most patient communication breaks down. Organizations invest in a patient portal because it checks a compliance box. Then they wonder why adoption stays low and readmission rates don’t budge.
Effective patient communication depends on the systems underneath it talking to each other. For Cortica, a value-based autism-care provider we have invested in alongside building their platform, we built a custom clinic operations platform that unified 18 legacy systems into one workflow. After that platform shipped, the organization’s waitlists moved from roughly six months to under 30 days, because scheduling, intake, and communication finally ran on a single source of truth.
How did CHLA solve NICU family communication?
Children’s Hospital Los Angeles partnered with Sidebench to build Baby Steps LA, a mobile application that replaced paper discharge packets with personalized, curated digital content for NICU families. The app has supported over 17,000 families, maintains a 4.7-star satisfaction rating, and won the American Hospital Association Innovation Challenge (3rd place, 2019), Fast Company Best Mobile Apps, and the w3 Awards Mobile App Gold Winner.
The core insight came from sitting in on discharge meetings. Not from a requirements document. Parents weren’t failing to absorb information because they didn’t care. They were failing because the delivery method ignored everything we know about how stressed people process information.
What Baby Steps actually does:
- Curated content library. Nurses help families select CHLA-approved resources during discharge, specific to their baby’s diagnosis. Not a generic packet, personalized materials.
- Baby profile. Stores diagnosis, physicians, medications, and care team contacts so parents can reference accurate details when talking to their pediatrician, pharmacy, or specialist.
- Interactive checklists. Post-discharge action items organized as to-do lists. Turn “remember to schedule a follow-up with neurology within two weeks” into a trackable, remindable task.
30,000+ downloads. Featured by Fast Company, winner of the American Hospital Association Innovation Challenge (3rd place, 2019), and a w3 Awards Mobile App Gold winner. But the number that matters most is the one you can’t easily quantify: families who went home feeling prepared instead of panicked.
How does IEHP communicate with 90,000 members across languages?

Inland Empire Health Plan (IEHP) partnered with Sidebench to build a member engagement platform that grew from 1,000 to over 90,000 active digital users within months, with no significant marketing spend, across a plan serving 1.5 million-plus members and thousands of providers in Southern California’s Inland Empire.
IEHP’s communication challenge was different from CHLA’s but equally specific. Their member population includes large Spanish-speaking communities, varying levels of digital literacy, and people navigating the overlap between Medicare and Medicaid benefits simultaneously. A standard patient portal in English with a translate button wasn’t going to cut it.
The platform shows each member exactly what they qualify for, in their preferred language, with clear next steps. Not a feature list. Not a benefits summary document. A guided experience that answers the question every member is actually asking: “what can I get, and how do I get it?”
1,000 to 90,000 users within months, with no significant marketing spend (see the full IEHP case study). That kind of adoption doesn’t happen with a generic portal.
What are the biggest patient communication mistakes?

The biggest mistake is treating patient communication as a training issue instead of a systems issue. You can train clinicians to make better eye contact and use simpler language. But if your discharge process still relies on a stack of paper and a five-minute verbal summary, training won’t close the gap.
Six mistakes we see consistently:
- Building portals nobody asked for. Patient portal adoption rates have hit 65% (ONC 2024), but access isn’t engagement. If patients log in once to check lab results and never return, your portal is a compliance checkbox, not a communication tool.
- Ignoring language barriers beyond translation. Running your English content through Google Translate isn’t multilingual support. Effective multilingual communication requires cultural context, reading-level awareness, and native-language content creation, not just word-for-word conversion.
- Assuming digital literacy. Not every patient has a smartphone. Not every patient who has a smartphone is comfortable downloading apps, creating accounts, and navigating menus. Your platform needs fallback channels: SMS, phone calls, printed materials generated from the same content system.
- Separating communication from workflow. If the nurse has to leave the EHR, open a separate system, and manually enter information to send a patient communication, it won’t happen consistently. Communication tools need to live inside the clinical workflow.
- Measuring the wrong things. Portal login counts and message open rates tell you about activity, not comprehension. Are patients actually following their care plan? Are readmission rates dropping? Those are the metrics that matter.
- Bolting on HIPAA after the fact. Patient communication platforms handle PHI by definition. HIPAA compliance needs to be built into the architecture from day one, not added as a security layer after development.
How do you measure patient communication improvement?

Measure patient communication through outcome metrics, readmission rates, care plan adherence, patient satisfaction scores, and comprehension assessments, not activity metrics like portal logins or message volumes. The goal isn’t more communication. It’s better understanding.
A practical measurement framework:
- 30-day readmission rate. The single clearest indicator that patients understood their discharge instructions and follow-up plan. CMS tracks this at the hospital level and applies financial penalties for excessive rates.
- Patient satisfaction (HCAHPS). The “communication with doctors” and “communication with nurses” domains in HCAHPS scores directly reflect patient perception. These scores affect CMS reimbursement.
- Teach-back completion rate. What percentage of patients can accurately describe their diagnosis, medications, and next steps before leaving? If you’re not measuring this, you’re guessing at comprehension.
- Platform engagement depth. Go beyond login counts. Track: content viewed by condition, checklist completion rates, time spent on educational materials, questions submitted through messaging. These tell you whether patients are using the tool to understand their care.
- Follow-up appointment adherence. Patients who understand why a follow-up matters show up for it. Track the gap between scheduled and completed follow-up visits.
The organizations getting this right aren’t just measuring whether patients received information. They’re measuring whether patients acted on it. That distinction is everything.
Key takeaways
- Communication failures contribute to up to 80% of serious medical errors, according to The Joint Commission on 2024.
- Miscommunication costs $1.7 billion in malpractice claims, with 1,744 patient deaths linked to communication errors (CRICO Strategies)
- Patient portal access hit 65% in 2024, but access doesn’t equal understanding. Purpose-built platforms outperform generic portals on every engagement metric (ONC/HINTS)
- Meet patients where they are, mobile-first, multilingual, integrated into clinical workflows. IEHP proved this by scaling from 1,000 to 90,000 users
- Measure outcomes, not activity, readmission rates, care plan adherence, and HCAHPS scores matter more than login counts
Sidebench perspective
We’ve built patient communication platforms across 50+ healthcare implementations, from NICU family support at CHLA to multilingual member engagement at IEHP. The pattern we keep seeing? Organizations invest heavily in EHR infrastructure and compliance systems but treat patient communication as an afterthought, a portal checkbox instead of a product. The technology matters, sure. But what matters more is starting from the right question. Not “how do we send patients information?” but “how do we make sure patients understand their care?” Those two questions lead to very different products. We’ve seen the difference across behavioral health, pediatric care, and health plan member engagement. Same principle every time.
FAQ
What is patient communication in healthcare?
Patient communication in healthcare covers every interaction where clinical information moves between providers and patients, from diagnosis explanations and treatment plans to discharge instructions and follow-up coordination. Effective patient communication means patients understand their condition, their care plan, and what to do next. It spans in-person conversations, digital tools, written materials, and multilingual support.
Why is patient communication important?
Communication failures contribute to up to 80% of serious medical errors, according to The Joint Commission. CRICO Strategies found that 30% of medical malpractice claims, representing $1.7 billion in costs and 1,744 deaths, involved communication breakdowns. Beyond patient safety, effective communication reduces readmissions, improves HCAHPS scores, and directly affects CMS reimbursement rates.
How can technology improve patient communication?
Technology closes the gap between clinical encounters by delivering personalized, condition-specific information through channels patients actually use, mobile apps, SMS, and patient portals. Effective platforms translate clinical data into actionable guidance, support multiple languages, integrate with EHR systems, and track whether patients understand and follow their care plans. CHLA’s Baby Steps app demonstrates this: 17,000+ NICU families supported with a 4.7-star rating.
What percentage of patients use patient portals?
In 2024, 65% of individuals accessed their online medical records or patient portal, up from 25% in 2014 (ONC/HINTS Survey 2024). App-based access grew from 38% in 2020 to 57% in 2024. Provider encouragement makes a significant difference: 87% of patients whose provider encouraged portal use accessed it, compared to 57% of those not encouraged.
How does poor communication affect patient outcomes?
Patients forget 40-80% of medical information immediately after a clinical encounter, and nearly half of what they do remember is incorrect (Kessels, 2003, Journal of the Royal Society of Medicine). This leads to medication non-adherence, missed follow-up appointments, preventable emergency department visits, and 30-day readmissions. The Joint Commission reported 1,575 sentinel events in 2024, with communication breakdowns cited as a systemic factor.
What is the HIPAA requirement for patient communication?
Any digital platform handling patient communication processes protected health information (PHI) and must comply with the HIPAA Security Rule (45 CFR 164.312). This requires access controls, audit logging, encryption, and transmission security at the application layer. A cloud provider’s BAA covers infrastructure, not the application-level controls needed for messaging, notifications, and content delivery to patients.
How do you improve patient communication in a hospital setting?
Start by identifying where communication breaks down, typically discharge, care transitions, and follow-up coordination. Then build or implement digital tools that: deliver personalized information based on the patient’s condition, support the patient’s preferred language, integrate into existing clinical workflows so staff actually use them, and measure comprehension rather than just delivery. Sidebench’s work with CHLA and IEHP followed this exact approach.
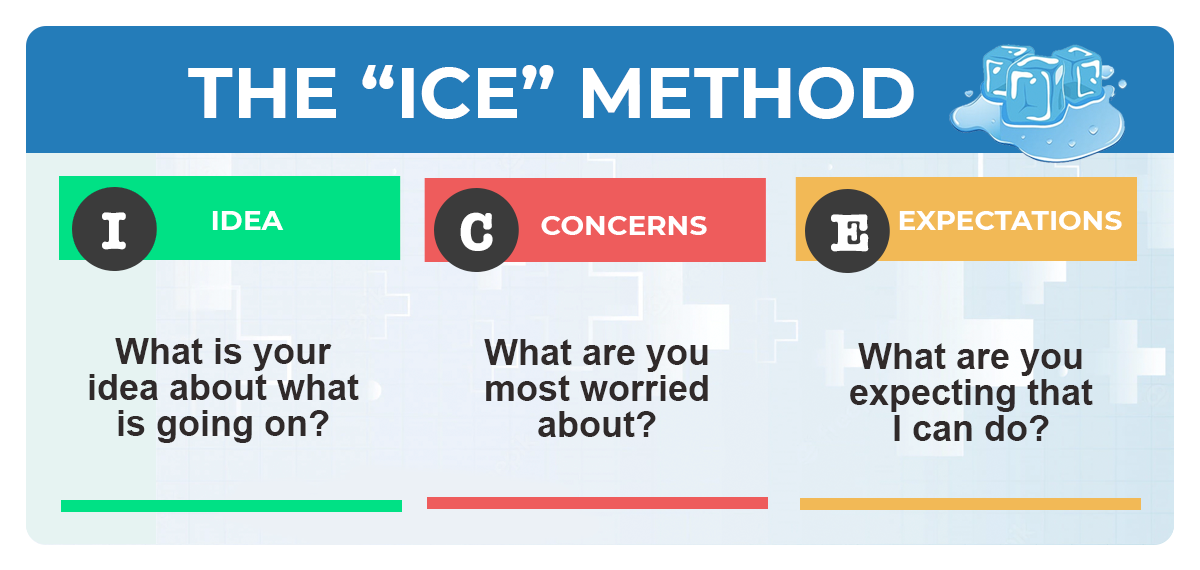
What are teach-back methods in patient communication?
Teach-back asks patients to explain their understanding of their diagnosis, medications, or care plan in their own words. It’s the only reliable way to confirm comprehension during a clinical encounter. Digital platforms can extend teach-back beyond the visit through interactive checklists, comprehension assessments, and condition-specific educational content that reinforces key information over time.
How does multilingual support affect patient communication?
Language barriers are one of the most common causes of patient communication failures. Simply translating English content isn’t enough, effective multilingual support requires cultural context, appropriate reading levels, and native-language content creation. IEHP’s member platform serves large Spanish-speaking communities in Southern California’s Inland Empire, and the bilingual design was central to scaling from 1,000 to 90,000 active users.
What patient communication tools are available for healthcare?
Options range from EHR-embedded messaging (Epic MyChart, Cerner Patient Portal) to standalone platforms (Klara, Luma Health, Relatient) to custom-built solutions for specific use cases. The right choice depends on your patient population, clinical workflow, EHR environment, and communication goals. Generic portals work for basic messaging. Complex use cases, like NICU discharge support or multilingual benefits navigation, typically require purpose-built platforms.
How do you measure patient communication effectiveness?
Focus on outcome metrics, not activity metrics. Track 30-day readmission rates, HCAHPS communication domain scores, care plan adherence rates, teach-back completion rates, and follow-up appointment attendance. Portal login counts and message open rates tell you about access, not understanding. CMS ties hospital reimbursement to several of these metrics, creating a direct financial case for measurement.
Measurable communication improvements show up in hard cost outcomes. For a national-scale medication-management company, the platform we built drove a 53% return on investment in hospital cost avoidance across more than 70 sites in 23 states, by putting a pharmacist-as-validator workflow and clear medication communication at the center of post-discharge care.
Can patient communication reduce hospital readmissions?
Yes. Research shows that follow-up calls within one week of discharge reduce 30-day readmissions by 19% for heart failure patients. Digital communication tools extend this effect by providing ongoing, personalized guidance between visits. The key is closing the loop, confirming patients understand their discharge instructions and flagging non-adherence before it becomes an emergency department visit.
Building a patient communication platform?
Whether you’re replacing paper discharge packets, launching a multilingual member portal, or trying to understand why your current platform has low adoption, the first step is understanding how your patients actually receive and process information.
Talk to the team that built CHLA’s award-winning patient communication platform →
Cited data sources
- The Joint Commission, Sentinel Event Data: 2024 Annual Review
- CRICO Strategies, Medical malpractice claims analysis: communication failures in 23,000 cases
- ONC/HINTS Survey 2024, Patient portal and smartphone health app access and use
- Kessels, 2003, Patients’ memory for medical information (Journal of the Royal Society of Medicine)
- IBM/Ponemon Institute, Cost of a Data Breach Report 2024
- CRICO/Candello 2024, Documentation errors and malpractice risk







